
Heather Nielson and Dr. Brent Feland, Physical Education
Proprioceptive neuromuscular facilitation (PNF) is a popular stretching method that increases flexibility. There are several different methods of PNF, but they all usually require the assistance of another person. The contract-relax method is a widely used PNF techniquei that utilizes maximum voluntary isometric muscle contraction (MVIC) followed by relaxation. An athletic trainer or therapist then pushes the relaxed muscle further into stretch after each contraction. So, traditionally the person is asked to contract the muscle being stretched as hard as possible in order to produce the MVIC. Very little research has been conducted to using submaximal contractions.ii iii Therefore, the purpose in our study was to determine if submaximal contractions utilized in contract-relax proprioceptive neuromuscular facilitation (CRPNF) of the hamstrings yield comparable gains in flexibility to maximal voluntary contractions.
A sample of 72 male subjects between the ages of 18 and 27 years was used for this study. Subjects qualified for the study by demonstrating tight hamstrings; defined as the inability to attain 80 degrees hip flexion during a straight-leg-raise. Sixty subjects were randomly assigned to one of three treatment groups: Group 1—20% maximum contraction, Group 2—60% maximum contraction, and Group 3—100% maximum contraction. The remaining 12 subjects were assigned into a control group (group 4) with no stretching. Subjects in groups 1-3 performed 5 separate 6-second CRPNF stretches at the respective intensity with a 10-second rest between contractions once per day for 5 days. Prior to and following the stretching, the subjects’ hamstring flexibility was measured using a Goniometer in a lying passive knee extension test. The 12 control subjects (group 4) were also measured twice daily for hamstring flexibility but did not perform any stretching trials.
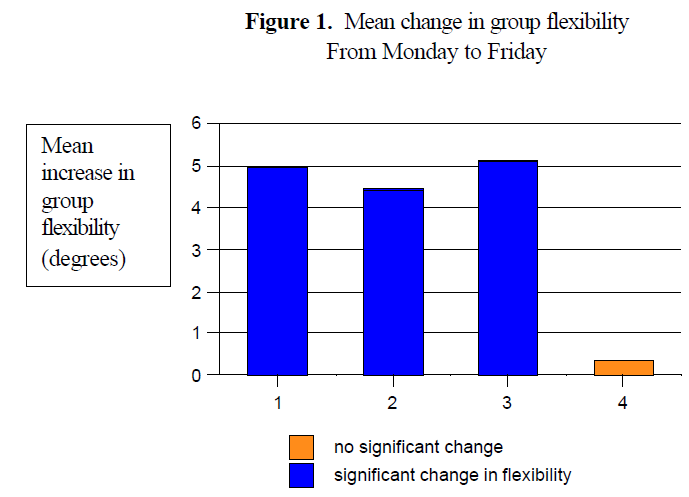
Paired t-tests were generated to determine if a significant change in flexibility occurred within groups by comparing the pre-test flexibility measurements on Monday to the flexibility measurements on Friday. The paired-t showed that groups 1, 2, and 3 exhibited a significant change in flexibility while group 4 did not significantly change. A graphical representation of the mean improvements in flexibility from Monday to Friday is shown in Figure 1.
The General Linear model ANOVA showed marginally insignificant (p=.056) differences between groups. However, pairwise comparisons using the least squared means did show significant differences between groups. All treatment groups (1,2,3) improved significantly over the g\control (group 4). However, there was no significant difference in flexibility gains between the treatment groups.
This study is important for improving the techniques of proprioceptive neuromuscular facilitation. It has long been standard to perform a maximal contraction in PNF techniques. However, maximal contractions put a person at risk for injury and delayed onset muscle soreness. The results of this study suggest that performing contractions at 20% and 60% MVIC are just as effective as 100% MVIC during CRPNF hamstring stretching. The results also verify that all interventions improved flexibility more than no stretching (control group). Although the max contraction group still showed greatest improvements overall, it averaged just .13 degrees greater flexibility than the 20% group.
Our results did show marginal insignificance int eh ANOVA general linear model. However, we believe that increasing the control subjects would have satisfied the insignificance by adding more power.
Therefore, our study has determined that utilizing submaximal contraction intensities of 20% and 60% MVIC in CRPNF hamstring stretching will yield comparable gains in flexibility as a 100% MVIC. The benefit of these findings can be beneficial to the therapist or trainer who would like to decrease the risk of injury and effect of delayed onset muscle soreness in the patient. The exact mechanism behind these results is unclear and future research should focus on finding neurophysiologic and anatomic explanations for the mechanisms behind these flexibility gains
References
- Smith CA. The warm-up procedure: To stretch or not to stretch. A brief review. Journal of Orthopedic Sports Physical Therapy. 1994;19(1), 12-17.
- Holt LE, Pelham TW, Campagna PD. Hemodynamics During a Machine-Aided Flexibility Protocol. Canadian Journal of Applied Physiology. 1995;20: 407416.
- Schmitt GD, Pelham TW, Holt LE. A comparison of selected protocols during proprioceptive neuromuscular facilitation stretching. Clinical Kinesiology. 1999;53: 16-21.