
Caden Duffy and Faculty Mentor: Alonzo Cook, Chemical Engineering
Introduction: Type 1 Diabetes (T1D) is an autoimmune disease that affects 1.25 million people in the United States, according to the American Diabetes Association. Although there are many short-term methods for regulating blood sugar levels, the only permanent cure for T1D currently is a pancreatic or islet transplant. This surgery is normally done to individuals with additional renal failure, as it is often performed in conjunction with a kidney transplant. With a large shortage of available pancreatic donors, we are developing alternative therapies to maintain normal blood sugar levels in individuals who suffer from T1D. Our current approach includes differentiating induced pluripotent stem cells (iPSCs) into pancreatic β-cells that can be transplanted, contained, and maintained to serve as a treatment for T1D. Although a few protocols for pancreatic β-cell differentiation have been published, we are investigating methods to create a cost-effective protocol which will have an increased yield of fully derived, insulin-producing pancreatic β-cells.
Methodology: For our studies, we use human iPSCs that are generated from peripheral blood monocytes with growth and expansion performed in Essential 8 medium. These cells are obtained through a collaboration that Dr. Cook has with the University of Utah. Cells are cultured using StemPro Accutase as a cell dissociation reagent, which allows the iPSCs to detach, enabling us to move them from plate to plate. We also use a Rho-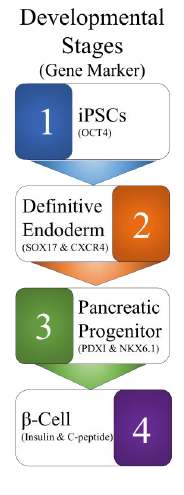 associated protein kinase inhibitor to improve the survival rate. The human iPSCs are differentiated into β-cells using a four-step process, as shown on the right. These steps include multiple different types of culturing medias, each containing various combinations of small molecules that have been shown to activate or repress the transcription of genes needed to mimic the normal pancreatic organogenesis. The medias must be optimized with several of these growth factors to induce expression of key genes, such as CXCR4, NKX6.1, PDX1, and C-peptide, at the proper time. We test for correctly differentiated cells under a light microscope, by performing fluorescence microscopy, and through using fluorescence-activated cell sorting (FACS). BYU currently owns a Becton, Dickinson FACSAria™ Fusion, which we have used previously to determine if our differentiation protocol is successful.
associated protein kinase inhibitor to improve the survival rate. The human iPSCs are differentiated into β-cells using a four-step process, as shown on the right. These steps include multiple different types of culturing medias, each containing various combinations of small molecules that have been shown to activate or repress the transcription of genes needed to mimic the normal pancreatic organogenesis. The medias must be optimized with several of these growth factors to induce expression of key genes, such as CXCR4, NKX6.1, PDX1, and C-peptide, at the proper time. We test for correctly differentiated cells under a light microscope, by performing fluorescence microscopy, and through using fluorescence-activated cell sorting (FACS). BYU currently owns a Becton, Dickinson FACSAria™ Fusion, which we have used previously to determine if our differentiation protocol is successful.
Results: Although we have previously completed a differentiation protocol using a commercially available kit for differentiating human iPSCs into pancreatic progenitor
cells, we have not yet achieved a reliable and reproducible method for differentiation of human iPSCs into insulin-producing pancreatic β-cells. Towards the beginning of this year, we experienced contamination with a few of the iPSC lines, which was discovered after their transportation from the University of Utah. After resolving this issue, the required materials for the cell culture medias were purchased. We proceeded with a first attempt of following a protocol. However, after a few weeks, we observed foreign cell morphology using light microscopy that did not correspond to what we expected with the differentiation protocol. Despite these setbacks, our work has brought forth unexpected positive results. Thanks in part to the ORCA funding, I was able to present our research at the Biomedical Engineering Society Annual Meeting in Phoenix, Arizona last October. While attending the conference, Dr. Cook and I had the privilege of meeting Dr. Quinn Peterson, a former BYU undergraduate who had recently completed his post-doctorate studies at Harvard, studying the differentiation of human iPSCs into insulin-producing pancreatic β-cells. Dr. Peterson discovered our lab through the conference agenda, and we met to discuss our work. Since this initial meeting, we have begun collaborating with him to improve our protocols. Recently, he has sent us his own differentiated insulin-producing pancreatic β-cells, which we hope to use as a guide for our own work.
Discussion: Since beginning our work with β-cell differentiation, we have had a number of setbacks. However, there are many areas in which we are improving. With the mentorship of Dr. Peterson, the enhancement of our protocol should be enabled. In our discussions, we have realized that we may need to better optimize our iPSC lines for pancreatic differentiation. Currently, we utilize iPSCs that have been optimized for studying cardiomyocyte differentiation because they have been the most readily available. This is due to the fact that multiple projects that are in Dr. Cook’s research lab use these cells. Originally, we did not expect this matter to make a significant difference in the outcome of studies, but it may be important to attempt our protocol with different cell lines, comparing the outcomes of each through analyzing differences in the cells using microscopy.
Conclusion: Many individuals are affected by T1D and could benefit from alternative therapies for regulating blood glucose levels. However, as expected when completing research with the use of any novel technology, there will be substantial barriers. We have successfully completed the differentiation of iPSCs into pancreatic progenitor cells in the past, but it has been difficult to replicate the process of differentiation into insulin producing β-cells. Despite past setbacks, and with the additional resources and advice which we have obtained thanks to our work this past year, we can continue the improvement of a pancreatic β-cell differentiation protocol. We expect to have the capability to produce glucose-stimulated, insulin secreting cells soon, which will allow us to further analyze encapsulation materials. Through the successful completion of a robust differentiation protocol and the further analysis of encapsulation materials, we will move forward in advancing the plausibility of an alternative therapy for the relief of those who suffer from T1D.