
John Heathcote and Dr. Josh West, Department of Health Science
The use of complementary and alternative medicine (CAM) has steadily become more widespread. For the first time, the use of traditional healers was included in the definition of CAM on the 2007 NHIS. Several Hispanic-specific CAM studies have included a variety of traditional healing and folk CAM therapies. Despite efforts to categorize CAM therapies, a common shortfall of many Hispanic- specific studies is the inclusion of prayer as a CAM practice. When included, the high prevalence of prayer has been found to greatly inflate estimates of CAM utilization.1 The tendency to include prayer in evaluating Hispanic CAM use might be expected as it has been noted that a fundamental aspect of Hispanic culture and spiritually is its interest in physical, mental, and spiritual healing.2 Religiosity is recognized as a multidimensional construct useful in measuring the degree of various religious behavior, belief, and spirituality. Degree of religiosity can be measured independent of religious sect, denomination, or tradition. The purpose of this study was to more fully understand the relationship between religiosity and both mainstream and traditional CAM use among a Hispanic population.
Data for this cross-sectional study were from 306 adult attendees at a free community health clinic that were recruited for participation in a self-administered survey. A trained bilingual (English/Spanish) research assistant distributed the self-administered survey. Utilization of CAM therapies was the dependent variable(s). Measures were adapted from Martinez, and included mainstream, traditional and total CAM utilization.3 Each construct was based on the question, “How frequently do you use [particular CAM therapy]: never (0), every 10 years (1), every 5 years (2), every year (3), every 6 months (4) or every month (5)?” Seven items were selected to represent mainstream therapies, and included massage therapy, aromatherapy, chiropractic, energy healing, megavitamins, homeopathy and acupuncture. Six items represented traditional CAM: herbal therapies, home remedies, spiritual healer, psychic and folk healer. CAM items were summed and used to construct three composite scales: mainstream CAM (Cronbach‟s alpha = .77), traditional CAM (Cronbach‟s alpha = .70), and total CAM (Cronbach‟s alpha = .77), which was a combination of both mainstream and traditional. Religiosity was measured with the widely used religiosity instrument developed by Rohrbaugh and Jessor.4
Most of the sample (71.8%) reported an annual income of $29,000 or less, 80.4% rented their residence, and only 34.6% reported having a steady job that provided a salary, while 24.2% were homemakers. Almost one-fifth (20.6%) of the sample was unemployed. The average religiosity score was 21.6 (SD = 5.9; RANGE = 1-30).
The average score for CAM usage of any type was 19.1 (SD = 8.8; RANGE = 1-67), traditional CAM was 7.5 (SD = 4.5; RANGE = 1-18), and mainstream CAM was 9.5 (SD = 4.7; RANGE = 1- 40). Home therapies, herbal remedies, traditional massages, use of megavitamins, and chiropractic care were among the most common forms of CAM therapies. Whereas all individuals were living in the US at the time of the survey, bivariate associations revealed that CAM usage varied significantly by country of birth. Significant differences emerged for total CAM and mainstream CAM where the highest reported use was among respondents born in South America. Females were significantly more likely to use traditional CAM than were males. Respondents that owned a home were more likely to use total CAM and traditional CAM.
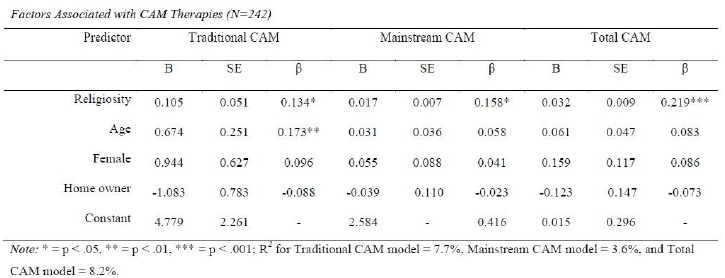
Multivariate regression was used to identify significant correlates of CAM utilization, after controlling for the potentially confounding influences of age and gender (See table below). Respondents that reported higher levels of religiosity also reported greater utilization of total CAM, traditional CAM and mainstream CAM. Interactions between religiosity and age, religiosity and gender, and religiosity and home ownership were also tested. The interactions were not significant and therefore excluded from the model.
The purpose of this study was to explore the relationship between religiosity and both mainstream and traditional CAM use among a Hispanic population. It was hypothesized that due to the spiritual nature of several traditional CAM therapies that traditional CAM would correlate with religiosity among the study population. This hypothesis was confirmed, as religiosity was positively associated with each type of CAM therapy. The current study adds support to the findings of McCurdy, who reported that families who consider themselves to be very religious are more likely to use CAM than those who self-reported as somewhat or not at all religious.5
We found participants of South American descent utilized mainstream CAM at significantly higher rates than those from Central America and Mexico. The current study found that participant age was significantly related to traditional CAM usage. The current study found that females utilize CAM therapies significantly more than males, although this finding was not observed in the multivariate analysis. Finally, the multivariate regression model in this study found increased religiosity to be associated with utilization of all three forms of CAM.
References
- Eisenberg, D., Kessler, R., Foster, C., Norlock, F., Calkins, D., & Delbanco, T. (1993). Unconventional medicine in the United States– prevalence, costs, and patterns of use. N Eng J Med, 328(4), 246.
- Magana, A., & Clark, N. (1995). Examining a paradox: does religiosity contribute to positive birth outcomes in Mexican American populations? Health Educ Behav, 22(1), 96.
- Martinez, L. (2009). South Texas Mexican American use of traditional folk and mainstream alternative therapies. Hisp J Behav Sci, 128-143.
- Rohrbaugh, J., & Jessor, R. (1975). Religiosity in youth: a personal control against deviant behavior. J pers, 43(1), 136.
- McCurdy, E., Spangler, J., Wofford, M., Chauvenet, A., & McLean, T. (2003). Religiosity is associated with the use of complementary medical therapies by pediatric oncology patients. J Pediatr Hematol Oncol, 25(2), 125-129.