
Alyssa Huber and David Miller with Dr. Brian Jensen, Mechanical Engineering
The purpose of our research was to create a tool to help in the treatment of hydrocephalus; hydrocephalus is a disease in which an obstruction causes a build-up of cerebral spinal fluid (CSF), a liquid found in the brain. Artificial shunts or passageways are used to relocate excess CSF in the treatment of hydrocephalus. Shunts are commonly misplaced, further aggravating patients’ symptoms. We developed an instrument, the CSF Sniffer, to increase the accuracy of shunt placement; it informs the neurosurgeon of the location of the instrument tip in the brain by measuring the intensity of light reflected off the brain. CSF is stored in ventricles, compartments in the brain. With the CSF Sniffer, the neurosurgeon can locate the ventricle and choose a place near to, but not touching the ventricle wall to place the shunt. Successful implementation of the CSF Sniffer will allow shunt placement to be more precise, yet less invasive. In skilled hands, this tool will benefit patients by minimizing potential complications.

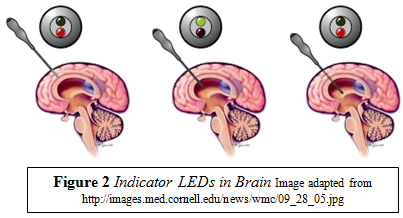
The ORCA Grant monies were used to supplement a project organized through the Department of Mechanical Engineering. Our team consisted of six students in the fields of mechanical engineering, electrical engineering, neuroscience, and industrial design. Additionally, we were mentored by a professor in the Mechanical Engineering Department, Dr. Brian Jensen, and a practicing pediatric neurosurgeon, Dr. Kim Manwaring. The final instrument is pictured in Figure 1. It is completely self-contained within an ergonomic handle, and has a two-color indicator on the cap. The final instrument is made of a surgical grade stainless steel tube with a light emitting diode (LED) at the tip; the sensor circuitry is inside the tube, and the external end of the instrument has the battery and the feedback indicator. The feedback indicator is two colored LEDs; one color, red, indicates that the probe tip is in white or gray brain matter, while the other indicator, green, turns on when the probe has breached the ventricle and entered into the CSF. As the shaft parts the brain tissue, the light is red; it switches to green once the ventricle has been penetrated, and then back to red at the opposite end of the ventricle (where it meets white matter). This is visually represented in Figure 2. This report will detail the progress made and significant events.
The project started as a question: how can the ventricle be differentiated from the rest of the brain? With that in mind, we began to research various methods of tissue identification. We found that tissue reflectance is a suitable macroscopic property to distinguish ventricles from the rest of the brain. In other words, we would capitalize on the different reflectance properties of brain tissue and the CSF stored in the ventricles. The principal components of the CSF Sniffer are the power supply (battery), the light source (white LED), the sensor (photoresistor), the feedback indicator (two colored LEDs), and the handle. Through consultation with neurosurgeons and medical professionals, we determined key specifications which required that the instrument be battery powered and disposable, as well as comfortable and compatible with existing surgical platforms. The shaft of the instrument is 5/32” in diameter, just small enough to fit within the 12 French diameter surgical tools. This makes the CSF Sniffer compatible with existing tools; surgeons are more likely to try it because it does not require a whole new surgical approach.
Inside the handle is a small, logical circuit that controls the light source and the feedback indicators. The circuit was the most difficult aspect of the instrument; we made seven generations of circuits before we worked out all the bugs. The circuit design required a coordinated effort between the mechanical and electrical engineers in the group in order to get everything to fit inside the handle, without minimizing performance. One of the problems encountered was that the indicator lights drain the battery too quickly; after several redesigns and a few component modifications, we were able to construct an instrument that works reliably over a long period of time.
The handle is the result of industry research. Initially eight handle designs were made and we surveyed medical professionals to find out which handle was the most comfortable, most similar to existing surgical instruments, and most likely to be adopted by surgeons. We selected the current handle based on the survey results; while it does not look like existing technology, it is comfortable and likely to be adopted by surgeons.
Our testing was rigorous; we found early on that the photoresistor that measures light intensity was not consistent. Drift experiments, experiments designed to judge how accurately the light intensity was measured, confirmed that the instrument was only good for about five minutes, after which it needed to be recalibrated. To remedy this problem, we implemented a more sensitive photoresistor and we incorporated a fiber optic cable into the design as well. The fiber optics act as a light guide, helping the light to travel directly to the photoresistor and not interfere with things in the steel shaft on the way to the photoresistor.
We cannot carry out medical tests of our prototype on human patients; however, we did create many test cells for our instrument. Our test cells included a sponge test cell, a Styrofoam model brain, and a tofu model. We have given our final CSF Sniffer prototype to Dr. Manwaring along with all documentation and he will continue instrument development and marketing in cooperation with Aesculap, a medical instrument manufacturer.