
Sgro, Jordan
Relationship Quality as a Predictor of Eating Disorder Symptoms and Body Image Perception in Women
Faculty Mentor: Dr. Wendy Birmingham, Psychology
Introduction
Eating Disorders (ED) are recognized as an important cause of morbidity and mortality in adolescents and adults and are much more common in women than in men. Women may exhibit ED symptoms but not be clinically diagnosed. Research has shown that individuals who exhibit sub-clinical eating disorder symptoms may eventually develop full syndrome. Thus, sub-threshold ED women are at increased risk but remain undiagnosed. Our culture often values women for their appearance, and this message is continually sent via media and other social institutions (e.g., religion), but having a supportive spouse can help buffer the negative messages women receive. While research has demonstrated the health protective benefits of marriage, research has also clearly shown that the quality of the marriage matters. Supportive marital relationships may buffer the effects incoming negative messages may have on a woman’s body image and eating behavior. However, relationships that are less supportive may not offer this same protection. Understanding the processes by which marital relationship quality (RQ) may impact ED behaviors can pave the way for interventions to improve marital RQ and decrease ED. A better understanding of the process also has implications for clinical practice by informing providers about the broader context of RQ and ED, which may be important in creating a plan of care. This study was an examination of the association between marital RQ and eating disorder (ED) behaviors in married women who had not yet been diagnosed with an eating disorder but were already showing symptoms of eating disorder behavior (“sub-threshold”). This study was unique in this aspect as no other study that we are aware of has assessed marital RQ in relation to eating disorder symptomology in sub-threshold women.
Methods
Subjects were recruited through SONA, advertisements posted in married student housing on the BYU campus, and social media sites. All potential participants were screened through Qualtrics to determine eligibility (e.g., married and within the appropriate age range; no history of ED diagnosis). “Sub-clinical” status was determined with the SCOFF questionnaire, a validated measure of ED behavior. Demographic and relationship information was obtained and women were scheduled for a one-on-one interview with a study research assistant. To ensure that we obtained a more representative sample, one co-investigator spent several weeks in Las Vegas where she recruited women from the LV area via Social Media (FaceBook). Recruiting in LV allowed the co-investigator to focus on older (i.e., older than college age) women. All other participants were recruited from the Provo-greater SLC area. In total, 62 married women were recruited to participate. At the interview session, we collected blood pressure readings and participants participated in a 30-40 minute interview. Interviews were recorded and uploaded to our secure server. Participants were paid $30 in cash or SONA credit. The total study commitment time was approximately 60 minutes.
Analysis
Descriptive analyses of questionnaire items were conducted using SPSS software version 23. Frequencies, percentages and measures of central tendency were calculated. Interviews were transcribed verbatim by one research team member and verified by a second. Coding of interview transcripts was conducted using NVivo11 software (QSR International Pty Ltd. Version 11, 2010). All interview transcripts were reviewed by the study PI and a grounded theory approach was used allowing codes, concepts and categories to emerge from the data. All transcripts were independently coded by two research team members, line by line. Agreement on coding was reached through close communication and frequent reviews. BAS responses were dichotomized into positive/negative or weight-related/non-weight-related. Body image responses were coded as positive, negative, or neutral.
Results
Participants were all married women and ranged in age from 21-47 with a mean age of 26. Average length of years married was approximately 4.8 years. Most were white (77.4%), had at least some college background (62.9%), and reported an income of $50,000 or less (78.9%).
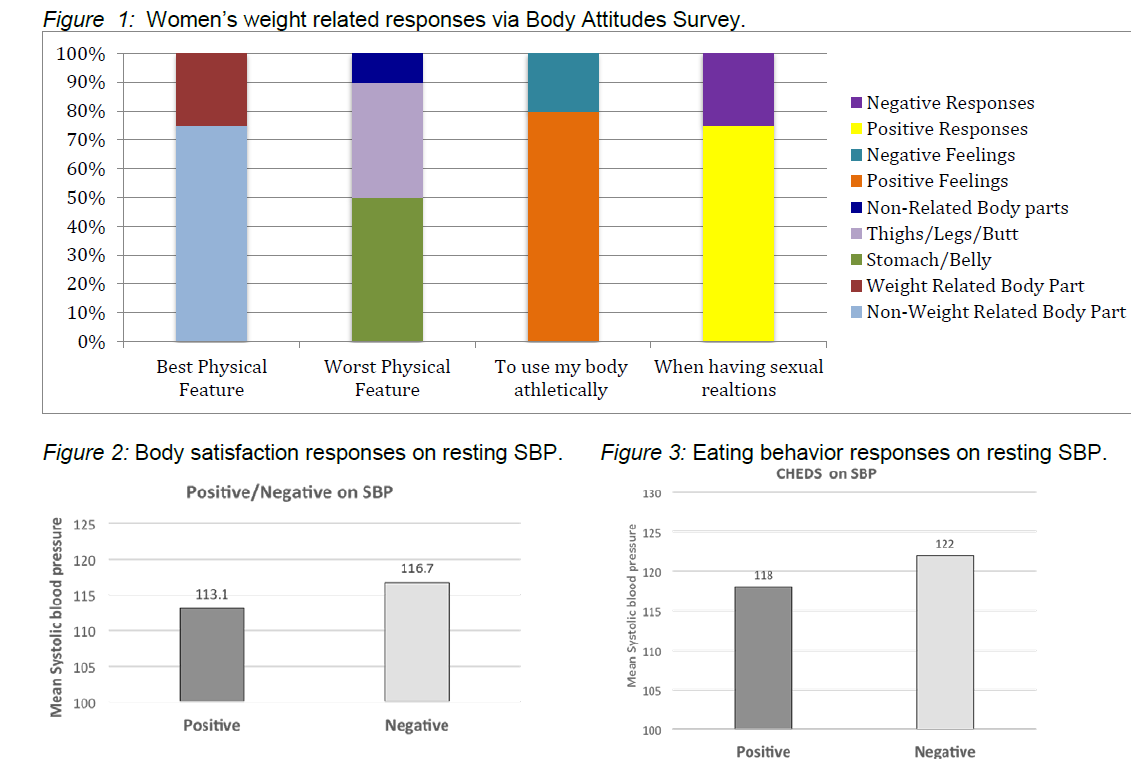
Body Satisfaction via Body Attitudes Survey (BAS): In response to the fill-in response question on the BAS “My best physical feature(s) is (are)”, 75.8% of our sample named a non-weight related body part, such as eyes, hairs, smile, lips, hair color, height, hands, and lungs. In response to the question, “My worst physical feature(s) is (are)”, about 50% named the stomach/belly area, about 40% named the thigh/legs/butt area, and only about 10% named a non-related weight body part. In response to the questions “To use my body athletically makes me feel”, nearly 80% indicated positive feelings (strong, more alive, happy, energetic, hopeful, capable, awesome, empowered, etc.) while about 20% had negative feelings (tired, inadequate, weak, out of shape, etc.). In responses to the item “If I am engaged in sexual relations, I feel _______ about my body”, almost 75% reported positive words (confident, good, appreciative, sexy, wanted, comfortable, etc.) and
about 25% reported negative feelings (insecure, self-conscious, embarrassed, etc.). All responses were coded through the NVIVO coding system. See Figure 1.
Marital Assessment Test (MAT): As marital quality increased, body satisfaction during sexual activity increased (B=-2.033, SE=.93, p=.029). Additionally, as marital satisfaction increased, overall body satisfaction increased (B=-.013, SE=.004, p=.003). Relationship quality was also associated with eating disordered thoughts, feelings, and behaviors, such that worse relationship quality was associated with higher reporter ED thoughts, feelings, and behaviors (B=-34.2, SE=10.5, p=.002).
Body Satisfaction on resting SBP: Blood pressure was examined with responses to the BAS questions: “When I see myself nude in the mirror, my reaction is…” and “In general, a word or phrase which best describes my feelings about my body is…”. Positive responses were associated with lower SBP and negative responses were associated with higher SBP [B=3.637, SE=1.68, p=.035]. See Figure 2.
Eating Behavior on resting SBP: Blood pressure was examined via the Change in Eating Disorder Symptoms Scale (CHEDS). Positive responses were associated with lower SBP and negative responses were associated with higher SBP [B=8.678, SE=3.812, p=.028]. See Figure 3.
Discussion and Conclusion
Our results indicate that sub-clinical women are struggling with body satisfaction issues especially when viewing their bodies. Sub-clinical women had a more positive view of their bodies when thinking of their bodies in motion, or action rather than being viewed. We also found that marital quality can affect body dissatisfaction and eating behavior in sub-clinical women. Of further importance, both eating behavior and body satisfaction impacted systolic blood pressure. The limitations of our study are that we had a small sample, and most of our participants were white and educated. Further research should examine ways to improve marital quality not just in clinically diagnosed women but in sub-clinical women as well. Further research should also examine ways to help sub-clinical women view their bodies’ capabilities, rather than focusing on appearance.