
Diana Snyder and Professor Beth Cole, Nursing
Main Text
Grief and bereavement can be defined as experiences created by responses to the loss of a family member or close friend. Such distressing experiences can be amplified by sleep dysfunction because of the devastating effects poor sleep quality has in healthy functioning. In a study done by Richardson, Lund, Caserta, Dudley, and Obray (2003), it was noted that 50 % of a group of 192 bereaved widows and widowers reported sleep disturbance within the first few months after the death of a spouse. Sleep disturbances have been highly correlated with problems such as depression, emotional lability, anger, loss of control, gastrointestinal upset, visual motor changes, large and fine motor disruptions, etc. Grief has been determined to affect sleep quality, which in turn affects immune function and overall health (Lorton et al., 2006). After reviewing many studies, grief appeared to affect the whole population from the young to the old. Though they may have created different experiences from their loss, studies have found a common prevalent factor of poor sleep quality amongst the varying populations. However despite these findings, Monk, Germain and Reynolds (2008) concluded that sleep dysfunction has been ignored clinically as it is not classified as a symptom of grief.
This study focused on how many grief group members identified sleep as an area affected by their loss. In addition, the participants’ sleep was evaluated after eight weeks, three months and six months to track sleep improvement. Drawn from the results of the study done by Richardson, et al. the current study hypothesized that at least 50% percent of grief members would report sleep as an area affected by their loss. A second hypothesis was that members would show improvement in sleep quality over the eight week, three month, and six month time period. This population included any bereaved individual age 18-80 and persons specifically searching for help in dealing with their grief by voluntarily signing up for a grief group program. Such information is useful in providing better treatment options for grieving victims of diverse backgrounds seeking for help to achieve better health and functioning.
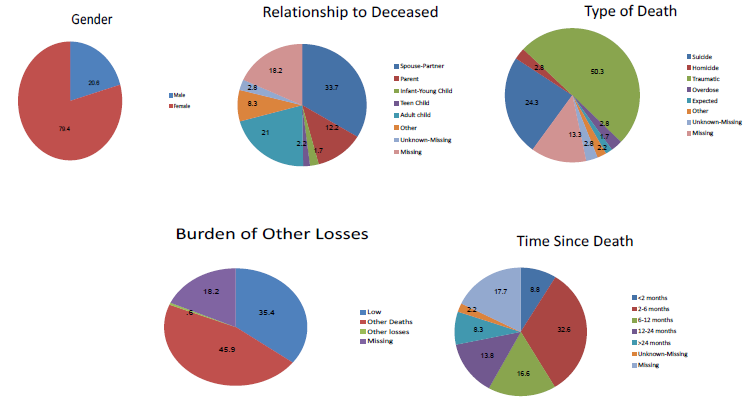
The demographics of the population (see Demographics below) showed that the majority were female (79.4%), someone who had lost a spouse (33.7%), a traumatic death (50.3%), people who were burdened with other deaths (45.9%), and people who had experienced the loss within 2-6 months (32.6%). The results of this study showed that of the 130 respondents; N =33 (25.38 %) reported sleep difficulties as an area of distress. Sleep difficulties were the most frequently reported somatic symptom chosen from the other choices of poor general health, poor appetite, or overall stress. In the overall reported areas of distress, sleep difficulty was the third most common response. There were eight point five percent that reported sleep problems had profound negative impact on ability to grieve, work performance and relationships. Of the 130 respondents, 33 of those who reported sleep dysfunction were tracked over six months to evaluate sleep improvement. Of the 33, 56% reported improvements at the end of the eight week group. Sixty one percent reported improvement at three months follow up and 72% reported improvement at six months follow up. These numbers were drawn from the questionnaires distributed at the first day of group, the last day of the grief group, and three months after and six months after. All responses were compared to the questionnaire given the first day of group. The data collected was preliminary and should be finished by the summer of 2010, which will include 230 respondents instead of 130 thereby strengthening the results statistically. Improved sleep function was associated with making healthy choices such as eating well and exercising while persistently poor sleep was associated with yearning for the deceased, stated loneliness for deceased, and the type of loss, widows and widowers being the most highly affected group.
From the results, it has been concluded that the overall population of grief victims does not appear to have as high a rate of sleep dysfunction as widows and widowers. Additionally, sleep improved because of a maturation effect, an effect defined by this study as the body striving to return back to normal functioning, the functioning level maintained prior to the loss. Lastly, this study concluded that for those whose sleep is inadequate and showed no improvement over six months or greater, they should be referred for further psychological and physiological evaluation. Future research can identify purposes for a higher sleep dysfunction in widows and widowers. Additionally the best treatment options of sleep dysfunction should be evaluated. Other potential studies can also look at associations with the demographics and the reports on sleep quality. These findings were presented at the Utah Conference of Undergraduate Research.
Demographics
References
- Lorton, D., Lubahn, C. L., Estus, C., Millar, B. A., Carter, J. L., Wood, C. A., & Bellinger, D. L. (2006). Bidirectional communication between the brain and the immune system: Implications for physiological sleep and disorders with disrupted sleep. Neuroimmunomodulation, 13(5-6), 357-374
- Monk, T. H., Germain, A., & Reynolds, C. F. I.,II. (2008). Sleep disturbances in bereavement. Psychiatric Annals, 38(10), 671-678. doi:10.3928/00485713-20081001-06
- Richardson, S. J., Lund, D. A., Caserta, M. S., Dudley, W. N., & Obray, S. J. (2003). Sleep patterns in older bereaved spouses. Omega: Journal of Death and Dying, 47(4), 361-383.