
Seth Spencer and Dr. C. Brock Kirwan, Psychology
Introduction:
Many studies have shown a correlation between physical exercise and healthy cognitive processing. It has been shown extensively that regular exercise has a positive impact on brain health. One example is a study that linked increased exercise with greater performance on as shown via a Stroop Color-Word test [1]. Similarly, regular exercise has been shown to be related to improved memory and object recognition [2]. Another study has shown that even a single session of exercise can alter functional connectivity in the brain as measured by the resting-state fMRI [3]. The problem with this literature is an utter lack of universal standards that constitute exercise. Most studies split a group of individuals into “high” and “low” exercisers. Sometimes the “high” exercisers are Olympian athletes—an impractical standard of exercise for the general public. This study has used the standards of exercise set forth by the American Heart Association (AHA) to provide a common convention for a scattered field of literature. To our knowledge, no previous studies have examined specifically how meeting the physical activity guidelines prescribed by the American Heart Association impact cognitive function. While we are currently aware that increased exercise benefits cognition, no previous studies have established an optimal level of that exercise. Our research addresses whether the guidelines of the AHA are sufficient to create a significant improvement in brain health.
Methods:
The participants of this study are adults age 18-40. Participants first complete an exercise questionnaire and then complete a memory task during an fMRI scan. Participants have been divided into three groups: (a) those who meet the standards recommended by the American Heart Association, (b) those who are substandard (engage in physical activity, but do not meet requirements), and (c) those who are sedentary.
The memory task was developed by Dr. Brock Kirwan and has been well-validated [4]. Each participant is shown a series of 642 images separated into six blocks. Throughout the sequence, some images are repeated; others are not repeated exactly, but have slight differences. Participants indicate whether each image is a new image, a repeat image, or an image similar to one that was already seen. This task places a large demand on the hippocampus to discriminate between very similar details. A score was created for each participant based on the percentage of correct responses.
In addition to participants’ behavioral responses, the fMRI measures the size and activation of the greater hippocampal subfield. A deconvolution analysis is used to normalize the data from participant to participant and individual voxels (group of cells which appear on the functional brain image) are adjusted for cross-subject comparisons. The neural activation in response to old images is subtracted from the neural activation in response to similar images. This yields a signal reflecting the neural costs associated with memory specificity.
Results:
Currently, 25 of 60 participants have been processed through the study. 3 males in the sedentary group, 5 males and 5 females in the substandard exercise group, and 7 males and 5 females in the exercise group which meet the AHA recommendations. We are near completion of recruiting the goal of 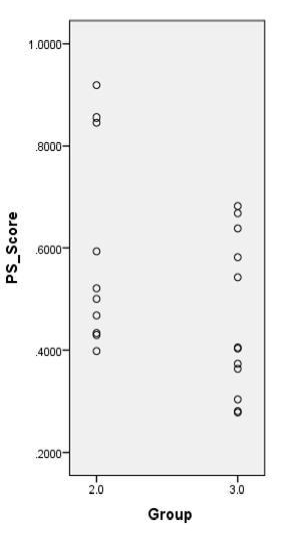 60 participants. A number of people are still needed in the sedentary group. Behavioral data from the current participants was evaluated using a one way ANOVA test. The sedentary group was excluded at this time because of such a small number of participants. In comparing the substandard exercise group (2) and the group which met the qualification of the AHA (3) a trend was seen toward significance with a p = 0.085, but is not significant at this time (Figure 1). It is interesting to note in the scatter plot that those in the substandard group had a wider range of scores than those in the exercise group. It is expected that a clearer difference will be seen when the data from the remaining participants has been collected, processed, and analyzed. The fMRI data will be analyzed when the data from all the participants is ready for processing.
60 participants. A number of people are still needed in the sedentary group. Behavioral data from the current participants was evaluated using a one way ANOVA test. The sedentary group was excluded at this time because of such a small number of participants. In comparing the substandard exercise group (2) and the group which met the qualification of the AHA (3) a trend was seen toward significance with a p = 0.085, but is not significant at this time (Figure 1). It is interesting to note in the scatter plot that those in the substandard group had a wider range of scores than those in the exercise group. It is expected that a clearer difference will be seen when the data from the remaining participants has been collected, processed, and analyzed. The fMRI data will be analyzed when the data from all the participants is ready for processing.
Discussion:
The imaging component of this study is critical so that we can understand whether the beneficial impact of exercise on memory is due to structural differences in the hippocampal region, functional differences, or both. Functional differences arise from microscopic changes in synaptic connections that are easily created and eliminated. If the hippocampus functions differently across groups, but doesn’t structurally look different, this would suggest that the benefits of exercise on cognition are relatively short-lived. Structural differences would suggest that the cognitive changes due to exercise are more robust and longer-lasting.
This study will help to open doors for future research looking at prescribed exercise guidelines and their relation to cognitive health. As our results are further developed we anticipate that this research will help institute a more practically-useful operational definition for studies with a similar goal.
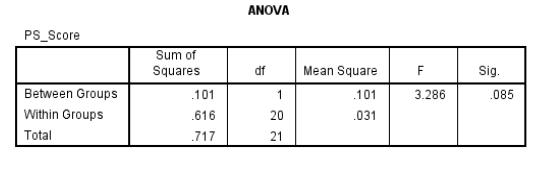
Figure 1
Sources
- Vasques PE, Moraes H, Silveira H, Deslandes AC, Laks, J. (2011) Acute exercise improves cognition in the depressed elderly: the effect of dual-task Clinics. Clinical Science [Sao Paulo] 66(9):1553–1557.
- Hopkins ME, Davis FC, VanTieghem MR, Whalen PJ, and Bucci DJ. (2012) Differential Effects of Acute and Regular Physical Exercise on Cognition and Affect. PMCID: PMC3374855 Neuroscience. 215: 59–68.
- Rajab AS, Crane DE, Middleton LE, Robertson AD, Hampson M, MacIntosh BJ. (2014) A single session of exercise increases connectivity in sensorimotor-related brain networks: a resting-state fMRI study in young healthy adults. Frontiers in Human Neuroscience, v.8: 625. PMC4132485
- Shelton DJ, Kirwan CB. (2013) A possible negative influence of depression on the ability to overcome memory interference. Behavioral Brain Research, 256, 20-26.
1 The AHA recommends at least (a) 30 minutes of moderate-intensity aerobic activity 5 days per
week OR (b) 25 minutes of vigorous aerobic activity 3 days per week and moderate-intensity
muscle-strengthening 2 days per week.