
David Walker and Dr. Michael Larson, Neuroscience
General anxiety disorder (GAD) affects approximately 5% of the U.S. population (Stein, 2009) and is the second-most frequent psychiatric disorder, after depression, in primary care settings (Wittchen & Hoyer, 2001). Although diagnosis requirements for GAD are extensive, common characteristics are hyper-vigilance, which is manifested as excessive or unreasonable worry, along with tension, fatigue and headaches (National Institute of Mental Health, 2010). These symptoms of excessive anxiety have been associated with increased rates of physical illness (Bowen, Barale, & Senthilselvan, 2000), a decline in cognitive processing abilities (Castaneda, Lonnqvist, Marttunen, Suvisaari, & Tuulio-Henriksson, 2008), and can become disabling (National Institute of Mental Health, 2010). The National Institute of Mental Health indicates that close to 40 million American adults are affected by anxiety disorders each year (Kessler, Chiu, Demler, & Walters, 2005); however, despite its serious nature and prevalence, as of yet, no physiological marker exists for diagnosis and little is known about the neural processes underlying GAD. This study tested the hypothesis that individuals with GAD would show a hyperactive electrophysiological response to error commission relative to demographically-matched controls.
We used scalp-recorded electroencephalogram (EEG) to measure the brain’s small electrical signals. We were interested in analyzing the event-related potentials (ERPs), the brain’s electrical output correlated in time with the presentation of external events. We used the flanker task, which consists of a series of arrows flashed on a screen in rapid succession, to elicit the ERPs. We were particularly interested in a specific component of the ERP called the error-related negativity (ERN).The ERN is a negative deflection in the event-related potential that occurs within 100ms after the commission of an error. The most prevalent theories hypothesize that the ERN is caused by mechanisms for detection of simultaneous activation of correct and incorrect neural representations, detection of errors, or an emotional response to errors (Botvinick, Cohen, & Yeung, 2004). In addition, because the ERN reflects trait and not state related symptoms, it has been proposed that the ERN would be a good marker for studying psychiatric disorders (Olvet, & Hajcak, 2008). Thus, we analyzed the ERN values of GAD participants and control participants to compare their neurological processing.
We tested our hypothesis that individuals with GAD would have increased ERN amplitudes in comparison with demographically-matched healthy control participants. Participants with GAD were diagnosed by a psychologist, psychiatrist, or physician in the community. The diagnosis was verified by using the MINI International Neuropsychiatric Interview at the time of study participation (Sheehan, Amorim, Baker, Dunbar, & Hergueta, et al, 1998). Individuals with GAD also took the Penn State Worry Questionnaire (Meyer, Borkovec, Metzger, & Miller, 1990) and State-Trait Anxiety Inventory (Speilberger, Gorusch, Jacobs, Lushene, & Vagg, 1983) to quantify anxiety symptoms. Following questionnaire and interview completion, each participant completed a computerized flanker task while we collected data from a 128-channel EEG system. The flanker task consisted of a series of arrows where participants were asked to respond as quickly and accurately as possible which direction the middle arrow was pointing. If it pointed to the left, they were to respond with their index finger, and if the middle arrow pointed to the right they were to respond with their middle finger. Four flanker arrows were first presented for 80ms before the onset of the middle arrow, which was presented for 30ms. This was followed by a delay of 500ms before the onset of a new set of flanker arrows.
We included 17 individuals with GAD (2 males; 15 females). Their average age, 22.6 (SD: 5.48), and years of education, 14.3 (SD: 2.47) were matched to 17 control participants (2 males; 15 females). The average age of the controls was 22.4 (SD: 3.97) and years of education was 14.3 (SD: 1.16). Groups did not significantly differ in age, t(32) = .143, p = .89, or years of education, t(32) = .44, p = .97. For GAD participants, the average trait anxiety score was 54.5 (SD: 10.9), while for the controls the average trait anxiety score was 33.9 (SD: 8.67). Groups did significantly differ in amount of anxiety symptoms t(32) = 6.08, p < .001.
We conducted a 2-Group (GAD, Control) x 2-Accuracy (correct, error) ANOVA on ERP amplitudes to test the primary study hypothesis. The main effect of accuracy was significant, F(1,32) = 37.99, p < .001, indicating ERN amplitudes were more negative than the ERPs for correct trials. The main effect of group was non-significant, F(1,32) = 5.64, p = 0.02, showing the ERPs did not differ between groups collapsed across correct and error responses. The Group x Accuracy interaction was trend-level significant, F(1,32) = 3.81, p = 0.06, indicating disproportionate neural responses to correct and error trials as a function of diagnosis. The mean ERN amplitude (Figure 1) for the GAD group was -2.99 (SD: 2.34), and the mean ERN amplitude for the control group was -1.17 (SD: 2.05).
These findings give evidence to support the hypothesis that people with GAD have a hyperactive physiological response to error commission relative to psychiatrically-normal individuals. This hyperactive physiological response indicates that the people with GAD are more acutely aware of their errors, even subconsciously, and that their brains’ error-processing systems differ from psychiatrically-healthy individuals. Importantly, the ERN data indicates that people with GAD have brains with a different neurological makeup than do psychiatrically-normal people. This is the first physiological measure found that can distinguish between psychiatrically-normal individuals and people with GAD. Unfortunately, however, these results cannot be extrapolated to pinpoint the exact locations of the neurological differences. More research is needed to determine the neural processes affected in individuals with GAD. This information will be vital to be able to develop improved medical treatments for individuals with GAD. 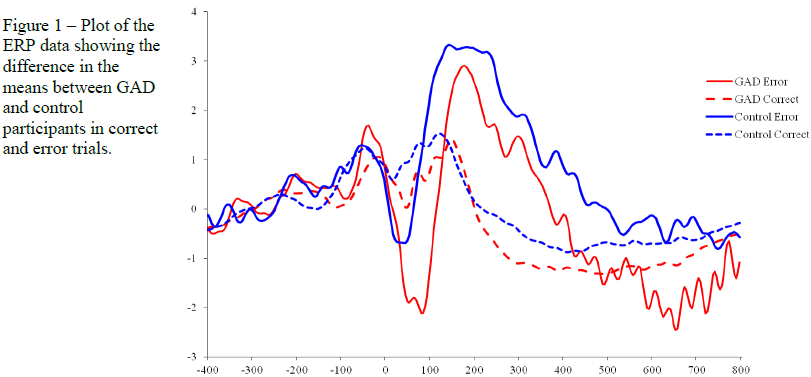
Scholarly Sources:
- Bowen, R.C., Barale, A., & Senthilselvan A. (2000). Physical illness as an outcome of chronic anxiety disorders. Canadian Journal of Psychiatry, 45, 459-464.
- Castaneda, A.E., Lonnqvist J., Marttunen, M., Suvisaari, J., & Tuulio-Henriksson, A. (2008). A review of cognitive impairments in depressive and anxiety disorders with a focus on young adults. Journal of Affective Disorders, 106, 1-27.
- Cohen, J.D., Yeung, N., Botvinick, M.M. (2004). The neural basis of error detection: conflict monitoring and error-related negativity. Psychological Review, 111, 931-959.
- Kessler, R.C., Chiu, W.T., Demler, O., & Walters, E.E. (2005). Prevalence, severity, and comorbidity of twelve-month DSM-IV disorders in the National Comorbidity Survey Replication (NCS-R). Archives of General Psychiatry, 62, 617-627.
- Meyer, T.J., Borkovec, T.D., Metzger, R.L., & Miller, M.L. (1990). Development and validation of the Penn State Worry Questionnaire. Behavior Research and Therapy, 28, 487-495.
- Olvet, M.O., & Hajcak, G. (2008). The error-related negativity (ERN) and psychopathology: Toward an endophenotype. Clinical Psychology Review, article in press.
- National Institute of Mental Health (NIMH): Anxiety Disorders. http://www.nimh.nih.gov/health/publications/anxiety-disorders/generalized-anxiety-disorder-gad.shtml. Accessed September 27, 2010.
- Sheehan, D.V., Amorim, P., Baker, R., Dunbar, G.C., Hergueta, T., Janavs, J., Lecrubier, Y., Sheehan, K.H., & Weiller, E. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59 [20], 22-33
- Speilberger, C.D., Gorusch, R.L., Jacobs, G.A., Lushene, R., & Vagg, P.R. (1983). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press. Stein, M.B. (2009). Neurobiology of Generalized Anxiety Disorder. Journal of Clinical Psychiatry, 70[2], 15-19.
- Wittchen, H.U., Hoyer, J. (2001). Generalized anxiety disorder : nature and course. Journal of Clinical Psychiatry, 62 [11], 15-19.