
Rachel L. Robison and Dr. William G. Pitt, Chemical Engineering
Prosthetic devices are commonly used in modern medicine. There are two types of prosthetic devices, implanted and transdermal. Implanted devices such as vascular grafts, heart valves, and prosthetic joints frequently become colonized by bacteria due to improper surgical techniques or post-operative infections.2 Transdermal devices such as catheters or electrical leads often become infected when bacteria from the patient’s skin migrates along the transdermal device and gains entrance into the body.1 If this occurs, microorganisms can cause serious infection at the site of the prosthetic device.
The infection of a prosthetic device is difficult to treat because the bacteria aggregate and adhere to each other and to prosthetic surfaces through their polysaccharide exudate. This exudate creates a sticky slime layer, or biofilm, that acts as a protective coatings for the microorganisms. These infections are difficult to cure because the organism is recalcitrant to antimicrobial treatment. The mechanism of recalcitrance is elusive, but is thought to reduce the amount of antibiotic able to penetrate and eliminate the microorganisms found in the lower layers of the biofilm.4 Since antibiotic treatment frequently fails to eliminate the entire biofilm from the prosthetic device, the current method of treatment is to remove the infected device and then treat the patient systemically with antibiotics. Once the infection is eliminated, another sterile prosthetic device is implanted in hopes that no further infection will occur.2
In an effort to develop a more effectual treatment for prosthetic infections, our laboratory explored the use of antibiotics combined with ultrasound as a means of eliminating these biofilms. Previously, our laboratory demonstrated that ultrasound potentiates the effects of antibiotics on in vitro (culture) bacterial growth.3 This increased activity of the antibiotic when combined with ultrasound is termed the “bioacoustic effect”. Realizing that ultrasound can enhance the activity of the antibiotic on planktonic cultures of microorganisms, we applied these findings to an in vivo (live) model.
Materials and Methods
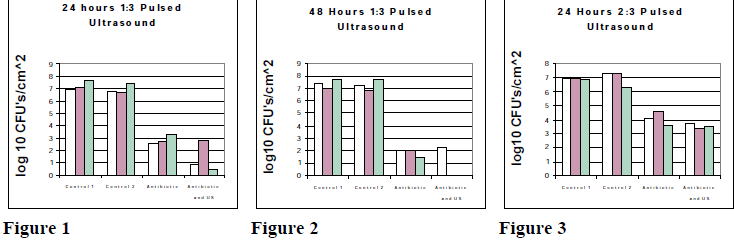
E. coli biofilms were grown on polyethylene disks. Four disks were used for each experiment. Two served as controls and two were implanted subcutaneously one disk on each side of the vertebral column of the rabbit. Immediately after surgery, gentamicin was administered systemically once every 24 hours. 24 hours post infection, ultrasound was applied to one of the two implanted disks. The ultrasound exposure lasted for the intensity and duration as specified for each experimental group. Initially the experiment was planned to explore parameters of 6, 12, 24, and 48 hour exposures to ultrasound. Initial results led us to focus on the 24 and 48 hour exposure times because bactericidal activity appeared to be most pronounced after these time intervals. For this reason, the parameters investigated were: 1:3 pulsed ultrasound with a peak waveform of 300 mW/cm2 and an average power density of 100 mW/cm2 exposed for 24 hours (figure 1). Another experimental group had the same ultrasound parameters except the exposure lasted 48 hours (figure 2). The third experimental group was a 2:3 pulsed ultrasound with a peak waveform of 300 mW/cm2 and the average power density was 200 mW/cm2 for a 24 hour exposure (figure 3). After ultrasound and antibiotic treatment, both polyethylene disks were removed from the rabbit. The disks were then stripped of bacteria by sonicating them in a 5% Trypsin solution. The bacteria were quantified through serial dilutions and each dilution was plated using the membrane filtration method.
Results
Figure 1 illustrates the 24 hour 1:3 pulsed ultrasound exposure. Two of the trials exhibited a pronounced reduction in viable organisms while one of the trials exhibited very slight reduction in viable counts. The mean viable counts for this experimental group were log10 2.65±0.42 CFU’s/cm2 for the non-treated side and log10 0.93±1.24 CFU’s/cm2 for the treated side. In two of the rabbits treated with 1:3 pulsed ultrasound for 48 hours there was complete killing of the biofilm. One of the trials from this experimental group exhibited larger counts on the treated side as illustrated in figure 2. Combining the results of all three trials gives the mean viable counts for the non-treated side as log10 2.01±1.16 CFU’s/cm2 and the treated side log10 0.75±1.30 CFU’s/cm2. Figure 3 illustrates the 2:3 pulsed ultrasound experimental group with a 24 hour exposure. This set of data exhibited the lowest bioacoustic effect with the mean viable counts for the non-treated side being log10 4.02±0.51 and the treated side was log10 3.56±0.19 CFU’s/cm2.
Discussion
Our data indicates that ultrasound has a bioacoustic when applied to bacterial biofilms in an animal model. This data indicates that 1:3 pulsed ultrasound for 48 hours exhibits the most pronounced bioacoustic effect. The 1:3 for 24 hours experimental group showed the next highest bioacoustic effect and the 2:3 pulsed ultrasound for 24 hours demonstrated the least amount of enhanced bactericidal activity.
References
- Pitt, W.G., M.O. McBride, J.K. Lunceford, R.J. Roper and R.D. Sagers. 1994. Antimicrobial Ag. Chemother. 38(11):2577-2582.
- Rediske, A.M., B.L. Roeder, M.K. Brown, J.L. Nelson, R.L. Robison, D.O. Draper, G.B. Schallje, R.A. Robison, and W.G. Pitt. 1999. Antimicrobial Ag. Chemother. 43(5):1211-1214.
- Rediske, A.M., W.C. Hymas, R. Wilkinson, and W.G. Pitt. 1998. J. Gen. Appl. Microbiol. 44:283-288.
- Sinisterra, J.V. 1992. Ultrasonics. 30:(3):180-185.
Acknowledgments
The author thanks Jared L. Nelson, John C. Carmen, Beverly L. Roeder, Andrea M. Rediske, Richard A. Robison, and William G. Pitt for their contributions to this research.