
Neal Peterson and Dr. Kirk Dearden, Health Science
Introduction
Over the last several decades in Latin America there has been a shift from exclusive breastfeeding (no foods or liquids other than breastmilk) to replacement feeding (foods and liquids in addition to or other than breastmilk). Whether because of social stigma or lack of time, mothers are increasingly turning to alternative feeding methods. Studies by various scientists have shown that exclusive breastfeeding is the most beneficial method of infant feeding and results in less sickness and decreased infant mortality. However, given that HIV can be transmitted through breastmilk, does the increasing prevalence of HIV globally significantly contribute to increased morbidity and mortality relative to deaths from diarrhea, acute respiratory infections and other infectious causes?
Hypothesis
The purpose of this study was to determine the negative consequences of sub-optimal feeding on infants in Latin America—because of deaths from HIV/AIDS and from other infectious agents. Using simulated models, the expected number of infant lives lost in Bolivia per 1000 live births was then quantified.
Methods
The data used for this study were obtained from the Demographic and Health Surveys (DHS)1. The DHS is administered in select countries globally and represents nationally representative data on maternal and child health. We used the 1998 DHS conducted in Bolivia. After downloading the data from the DHS web site, we checked it and cleaned it for additional analysis. We used SAS software (Cary, NC) for all data analysis, as outlined below.
For our analysis, we first categorized mothers into one of six infant feeding modes: breastmilk only; breastmilk and food; breastmilk and bottle; breastmilk, bottle and food; bottle only; and bottle and food. These 6 categories were derived by Burkhalter, who examined the scientific literature to evaluate relative risk of death for various feeding modes2.
After calculating the percentage of infants in each category, we collapsed feeding modes into three categories: full breastfeeding, any breastfeeding, and no breastfeeding. Data on percents of children who were fully breastfeeding, partially breastfed or not breastfed at all (by age of infant) were then entered into an Excel calculator written by Kirk Dearden with contributions of Ross and Burkhalter3. This calculator was based on assumptions concerning the rate of infant mortality, the number of infants born per year in Bolivia (255,000)4, and the HIV seroprevalence in Bolivia (.1%)5, as well as other assumptions about transmission of HIV/AIDS and relative risks of death for various infant feeding strategies including the MTCT rate before and during delivery (.24%), and the incidence of new cases among breastfeeding mother, MTCT rate during breastfeeding, mortality rates among non-infected and infected infants, and relative risks of mortality from non-HIV causes for each of the three infant feeding modes.
Results
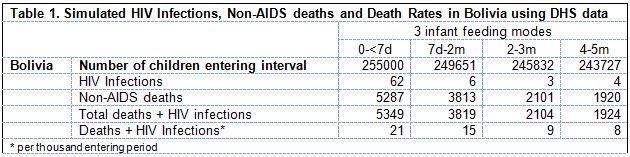
From the results of the simulation, currently in Bolivia, those infants who were given breastmilk exclusively were more likely to survive than those who were not exclusively breastfed. Because the prevalence of HIV in Bolivia is very low, the effect of HIV on the death rate of infants was not appreciable in relation to the number of deaths that could have been prevented by exclusive breastfeeding (see Table 1).
Challenges
One of the major challenges in this project was managing and preparing data for analysis. Many hours were spent sorting and discarding incomplete data. Furthermore, it was challenging to make assumptions regarding the behaviors of mothers and infants in Bolivia. In the future, it would be beneficial to compare these results with studies done in other countries.
At a programmatic level, while most mothers in Bolivia exclusively breastfeed, encouraging mothers to stop breastfeeding altogether when infants reach 6 months of age will be a considerable challenge.
Conclusion
From the data that were collected and the simulations run, it is apparent that the optimal feeding method for infants given the current prevalence of HIV in Bolivia is exclusive breastfeeding. When the infants were not exclusively breast fed, there were many more infant deaths due to non-optimal feeding than those who died from HIV. Therefore, policy makers and program planners and implementers can best decrease the number of infant deaths in Bolivia by encouraging exclusive breastfeeding for the first 6 months of life, followed by a complete cessation of breastfeeding (to avoid on-going exposure to HIV/AIDS through mother’s milk). Based upon these findings, staff from Private Voluntary Organizations and other non profits, as well as the Ministry of Health in Bolivia should be aware of the impact of different feeding methods on infant survival and implement policies accordingly.
References
- DHS Web site: www.measuredhs.org
- CALCULATOR for Nearness to Optimal Feeding Indicator; An Indicator of Community Feeding during the First Six Months of Life, Barton R. Burkhalter, December 2001.
- A Spreadsheet Model to Estimate the Effects of Different Infant Feeding Strategies on Mother-
to-Child Transmission of HIV and on Infant Mortality, Kirk Dearden, Jay Ross, Barton R.
Burkhalter. - Unicef Web Site: http://www.unicef.org/infobycountry/latinamerica.html
- HIV Seroprevalence data: http://www.who.int/GlobalAtlas/PDFFactory/HIV/EFS_PDFs/EFS2004_BO.pdf