
Marissa Miller and Dr. Scott Sanders, Sociology Department
Introduction
Liahona Children’s Foundation (LCF) is a faith-based community organization that seeks to “nurture the potential of children to lead healthy and productive lives by eliminating malnutrition and providing educational opportunities among LDS (Latter-day Saint) children and their friends”. They do this by providing health initiatives include growth monitoring and nutritional supplementation. They are piloting the use health education lessons. In this field study, I evaluated the LCF program and initiated a randomized control trial to test the effectiveness of the health education lessons. The purpose of the project is to assess the effects of nutritional supplementation and basic nutritional education on the health of malnourished children in the Philippines.
Evaluation Methods
This study is designed as a randomized control trial. After the Liahona Children’s Foundation selected the stakes, we held a screening to determine which children, ages 6 months to 5 years, were malnourished by taking height and weight measurements. To qualify for this program, children must be 2.0 standard deviations below the average HAZ (height for age z-score) or WAZ (weight for age z-score). These children will be eligible to receive nutritional supplements from the Liahona Children’s Foundation. From this pool of children, individuals who were eligible for the RCT were those who were not severely malnourished, had no chronic diseases or serious illnesses, were not already taking vitamins, and children for whom we received parental consent.
Parents/caretakers of the eligible children filled out a survey about their family and the child. The survey included questions regarding the child’s normal eating habits and behavior as well as household characteristics (size, income, educational background, parents’ occupation and age, etc.). Parents were also asked to provide a parental consent for the child to participate in the study. The anthropometric measurements and parent survey provided the baseline information for our main dependent variables: height, weight and nutritional educational compliance.
We then randomly assigned treatments from the pool of children eligible for the study. (This was done randomizing at the individual level.) We also randomized at the household level meaning that once one child from the household was randomly selected into a treatment group, all children from that particular household who were qualified were also selected into that same treatment group. In this study, researchers gave the entire household supplements once one individual was randomly selected. Children were assigned a 1 or 2 from a random number generator once their nutritional status was calculated and showed that they were malnourished. The groups are as follows: Treatment Group 1 – Nutritional supplement and nutritional education and Group 2 (Control) – Nutritional supplement only. Supplement distributions and educational classes are conducted monthly.
Results
Health Outcomes Based on Treatment
The research question of interest is testing the effects of the health lessons combined with nutritional supplements versus simply taking the supplements. This analysis is very preliminary as lessons were only administrated across all stakes in August, with only one month of lessons (most were taught the lesson on disposal of human waste) it would be very surprising to see any results in the differences of heights and weights between those children whose mother’s got that one lesson and those who did not. Because of the successful randomization of the treatment and control group interpreting the impact of the treatment is rather straightforward. Between the proper randomization and the Law of Large Numbers other variables should be equalized across both treatment groups, leaving just the impact of the treatment in the model while other variable are held equal.
*The following results are too preliminary for interpretation, but rather show how data analysis will occur as more data becomes available over time.
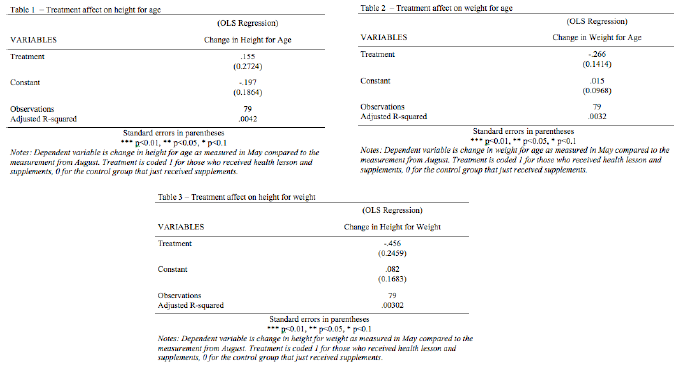
While the results lack statistical significance, a closer examination of Tables 1, 2, and 3 shows interesting indications. Table 1 indicates that the treatment helps improve the height for age compared to those who did not receive the health lessons. Table 2 indicates that the treatment actually worsens weight for age compared to those who did not receive the health lessons. Table 3 indicates that the treatment actually worsens height for weight compared to those who did not receive the health lessons. Again, these results are too preliminary for any conclusive results.
Discussion/Conclusion
No conclusions can yet be draw on the difference the treatment group makes. These first models show the dependent variable that we will continue to analyze as the study continues. These findings are also quite dependent on the attrition level, as these models each have very few observations in them, making results very unstable. If the attrition level can be improved and more lessons are taught overtime, these results should be more conclusive. Efforts by LCF to keep children coming back to each screening and to help coordinators accurately report results of those screenings will improve the interpretation of the treatment effect (meaning change in zscore between the screenings).