
Kyle Eversole and Wendy Birmingham, Department of Psychology
Introduction
Positive spousal support and relationships that are high in positivity are beneficial in terms of health-outcomes, including lower clinical and ambulatory blood pressure, an indicator of cardiovascular disease risk. Such positive relationships have been associated with lower mortality and morbidity. Conversely, relationships with more negative social interactions have been shown to cause high stress. This stress can cause both psychological and physiological problems, including higher resting and ambulatory blood pressure. In fact, some studies suggest that remaining single is more beneficial than a negative marriage or relationship. However, most marriages are not strictly positive or strictly negative, but rather, a mixture of both. So what does this mean for individuals whose marriage is high in both positivity and negativity (e.g., ambivalence) in terms of health outcomes? Can the positivity in the relationship offset the negativity in the relationship? That was the question we examined in this study. Our study examined the health consequences of ambivalent marriages (high in both positivity and negativity) versus more supportive marriages (high in positivity, low in negativity).
Methods
Our study goal was to recruit 100 couples for the study- so far, we have recruited 40 (n=80), and data on these 80 individuals will be used for this analysis. Couples were recruited via social media (Face Book, Instagram) and flyers distributed to married housing on BYU campus. Eligible couples were married for at least 2 years, living together with no other people (i.e., children) in the home. Both spouses were required to work outside the home, and had to have no history of cardiovascular disease, high blood pressure, and a BMI under 29.9. Eligible couples came to the lab and completed demographic questionnaires, health, social support, and relationship quality measures. They were then fitted with the monitors and instructed to wear them throughout the entire day until they woke up the next morning. With each reading participants were asked to fill out a short phone application-based survey (Daily Diary) that recorded what they were doing at the time of reading (standing, walking, talking with spouse or coworkers, if they had consumed any alcohol or stimulants, etc) One sample blood pressure reading and one Daily Diary entry was taken and completed before the participants left the lab to ensure participants understood the process. The next day, they removed the monitors, and returned the equipment to the lab, and were paid for their participation.
Analysis
Descriptive analysis of questionnaire items was conducted using SPSS software version 23. Frequencies, and percentages were calculated. PROC MIXED analysis was conducted using SAS 9.4. PROC MIXED analysis accounts for the interdependence between the couples. Because blood pressure tends to be lower at night (i.e., a good cardiovascular profile) we conducted initial analysis to determine the association between daytime and nighttime blood pressure and marital quality.
Results
Analysis focused on how ambivalent marriages affected physical health versus more supportive marriages. Among the 80 participants, 7 were excluded because their body mass indices were over 29.9. 45.2% (n=33) were male, 54.8% (n= 40) female. The mean age of these participants was 23.77 with a SD of +/- 2.37 and a range of 21-37. 19.2% made less than $15,000 yearly, while 42.5% made between $15,000 and $29,999, and 26% made between $30,000 and $49,000. The remaining .3% made $50,000 or more. 58.9% had some college, 28.8% graduated college, and 8.2% completed/attended graduate or professional school. Most (91.8%) report at least weekly church service or activity attendance, and 98.6% report being affiliated with the Church of Jesus Christ of Latter Day Saints. 15.1% of participants rated their health as excellent, 71.2% as good, and 13.7% as fair.
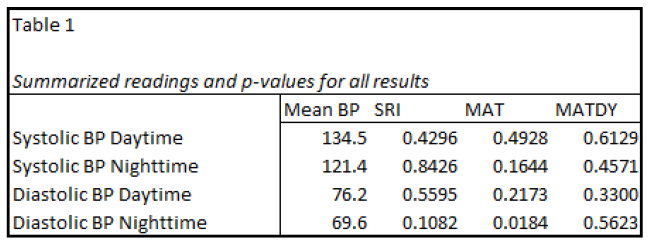
For the present analysis we used mean daytime systolic blood pressure (SBP) and diastolic blood pressure (DBP), a mean nighttime SBP and DBP. We examined the association between marital quality (ambivalence and supportiveness) and both daytime and nighttime SBP and DBP. We found no significant association for either daytime or nighttime SBP (daytime, p= 0.4296; nighttime, p= 0.8426 ) and DBP (daytime, p= 0.5595 nighttime, p= 0.1082) when factoring spousal support. We then examined marital quality in terms of a more unidimensional approach using the Marital Adjustment Test. We found significant results for the readings of nighttime DBP (p= 0.0184) such that better marital quality was associated with better nighttime DBP. We found no other results for daytime DBP or either daytime or nighttime SBP. (DBP daytime, p= 0.2173; SPB daytime, p= 0.4928; SPB nighttime, p= 0.1644). Lastly, we found no results for either daytime or nighttime SBP (SBP daytime, p= 0.6129; SBP nighttime, p= 0.4571) or DBP (DBP daytime, p= 0.3300; DBP nighttime, p= 0.5623). A summarized version of this data can be found in table 1.
Discussion and Conclusion
Previous studies have suggested that marital quality affects mortality and morbidity, and that married individuals have lower mortality and morbidity than their unmarried counterparts. Generally, research emphasizes that positive marital quality contributes to these health benefits. Likewise, it has been shown that marital stress has detrimental effects upon cardiovascular health. Most prior research has focused on either positive or negative relationships and their effects on health. This study intended to explore how martial relationship quality is associated with physiological health outcomes, specifically, blood pressure and in this analysis we used mean SBP and mean DBP readings. We found lower nighttime DBP associated with higher reported marital quality. However, our end analysis (i.e., at 100 couples) will be an examination of the contribution of each individual blood pressure reading rather than a mean. Additionally, we will examine nighttime blood pressure dipping, as a beneficial cardiovascular profile would include a SBP and DBP dipping of 15-20% overnight. This preliminary analysis only examined mean readings. We fully expect to find associations with ambivalence and worse daytime SBP and DBP, as well as less overall dipping in our final analysis. Our plan for the additional couples is to collect older couples to give us a richer view of marital quality and SBP and DBP.
Limitations include: we collected data for this study in Provo, where the average age was 23.77 and religious preference is Latter Day Saint. Our collection of older couples, and couples from outside the Provo area will give us a more generalizable sample. However, our analysis of forty couples of the projected one hundred couples does indicate that nighttime DBP is associated with marital quality.
Although I have graduated, I still plan to continue working with Dr. Birmingham in examining this data once it is all collected. We have high hopes that once all participants are processed and data examined, we will have a better idea of how ambulatory blood pressure, nighttime blood pressure dipping, and relationship quality are associated.