A Microfluidic Approach to Measuring Endothelial Cell Migration
Abstract
Pathological angiogenesis or new vessel growth plays a key role in a number of diseases including tumor growth and several eye diseases that can lead to blindness. While antiangiogenic therapies have been developed for many of these pathologies, there remains a pressing need for more effective anti-angiogenic therapy with fewer side-effects. Capillary morphogenesis gene 2 (CMG2) has been shown to play an important role in angiogenesis and is a potential target for future anti-angiogenic therapies. To better understand the physiological role of CMG2 and to accurately compare how well different CMG2 antagonists inhibit endothelial cell migration (the putative mechanism for how CMG2 functions as an antiangiogenic target), we have developed a more robust endothelial cell migration assay which is typically plagued by low precision and reproducibility.
Introduction
Angiogenesis, or neovascularization, is the process by which new blood vessels form from existing ones. This process is essential in fetal development and wound healing but is often pathological in adults. For example, inappropriate blood vessel growth in the retina causes diseases that can lead to blindness, including macular degeneration and diabetic retinopathy. In addition to its role in eye diseases, angiogenesis plays a key role in tumor growth and is one of the hallmarks of cancer. Current anti-angiogenic therapies include those that target vascular endothelial growth factor (VEGF). While they are effective at halting the progress of neovascularization, these treatments can also bring significant side effects—including hypertension and slower wound healing—and lose efficacy over time as alternate pathways to angiogenesis emerge. Thus, there remains a need for alternative targets for anti-angiogenic therapies. Capillary morphogenesis gene 2 (CMG2) is an integrin-like transmembrane protein that is a potential target for future anti-angiogenic therapies because it is known to play an important—though not well understood—role in angiogenesis.
Fundamentally, angiogenesis involves two processes: migration and proliferation. Endothelial cells migrate towards the source of pro-angiogenic signals, and proliferate as they go to form new vasculature. Thus, an anti-angiogenic therapy could presumably work by inhibiting migration, proliferation, or both simultaneously. My project was to develop a more robust migration assay to measure the effects that different CMG2 antagonists have on endothelial cells.
RESULTS: We first attempted to perform the traditional migration assays that one can find in the literature. When we were not able to achieve reproducible results with these, we turned to microfluidics. Following a design found in the literature, we fabricated our own y-shaped device made of polydimethylsiloxane (PDMS). After seeding the cells in the device and allowing them to grow to confluency, we flowed trypsin into one side and complete medium into the other. Ideally, this can be done under laminar flow so that a clean wound will be created as the trypsin solution causes the cells to detach from the bottom of one side of the device. In practice, however, we found it difficult to maintain the consistent flow requisite for a well-defined wound.
Although we planned to design and fabricate our own device that would essentially be a scaling up of our y-shaped device, a different possibility presented itself in the form of a commercially produced device acquired for use on another project (CellASIC ONIX; EMD Millipore). This is a semi-automatic microfluidic platform that allows us to precisely control the conditions that our cells experience. Cells are first seeded in the CellASIC device by flowing them into the device under laminar flow-like conditions so that they settle in the middle of the main channel. They are then allowed to adhere and spread for about 24 hours, though without
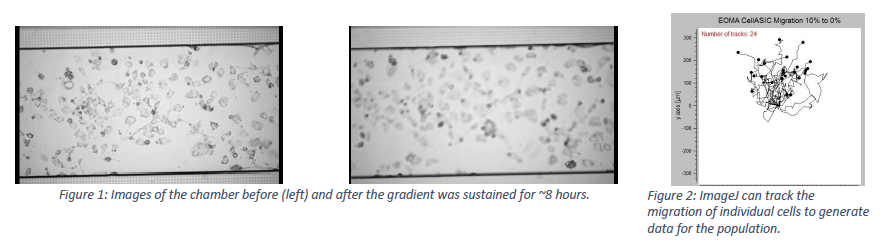
reaching confluence. To perform the assay, a gradient is created in the main channel by flowing two different solutions in the top and channels. A perfusion barrier separates these smaller channels from the main one. As the different solutions perfuse into the main chamber, a linear gradient is created and sustained throughout the duration of the experiment. During the extent of the experiment, an image was taken by microscope once every minute. These images together form a video that displays the cell behavior during while the gradient is established.
The images below demonstrate the success we have experienced with this new platform. Although the image went out of focus during the experiment, the cells generally migrated upward. This is the expected response because we flowed full-serum medium in the top channel and serum-free medium through the bottom. The video was then analyzed by a software which tracked the distance travelled by each cell throughout the video.
Despite this being a commercial produce, there have been no reports of suing this device for monitoring endothelial cell migration, rather it is targeted chemotaxis research. As we continue to develop this assay platform, we still need to optimize the protocol for cell density, flow rates, length of time-laps, and program a dose response curve into the assay while measuring assay performance.
CONCLUSIONS
The semi-automatic migration assay that we have started to develop by using the CellASIC ONIX system has clear advantages over its predecessors. It is not as manually-intensive, leaving less room for error by less-experienced users. It also allows us to control with greater precision the conditions of the experiment. Now that we know that we can cause the cells to migrate by establishing this gradient of nutrients, we will be able to compare how quickly they migrate when there are different treatments included in the medium.
FUTURE DIRECTION
For this to be a validated assay, we need to first show that it is repeatable. That is, we need to demonstrate that the cells migrate at about the same rate when we establish this identical gradient of full-serum to serum-free medium. If we can do this, we will then be able to compare how quickly the cells migrate while treated with PA, S16, and other molecules found to bind to CMG2. We aim to eventually find what the endogenous ligands of CMG2 are in hopes of discovering its physiological role in angiogenesis. These discoveries promise to provide significant insights into the complex process of pathological angiogenesis and may also lead to the development of more effective and less harmful therapies for those that suffer from angiogenic-dependent diseases.
AKNOWLEDGEMENTS
Ph.D. candidate Tsz Ming Jeremy Tsang contributed extensively to this research and to my understanding of it. Dr. Kenneth Christensen provided excellent mentoring and direction along the way. I was funded by BYU’s Office of Research and Creative Activities.